Innovative technology
to assist walking & improve mobility.



As reported in an earlier blog – dropped foot stimulation can significantly increase walking speed in stroke patients. Walking speed in stroke patients shows a wide variation depending on a # of factors including degree of motor loss from the stroke and time since onset of the stroke. In a study on walking speed after stroke […]
Read more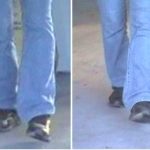
In patients post stroke or post onset of MS who demonstrate ankle dorsiflexion with preserved tibilais anterior function the principal gait deficit may be loss of ankle eversion due to peroneus longus & brevis paresis. The presenting gait feature is loss of a normal plantagrade foot position during & at the end of swing phase of […]
Read more
Flexion synergy in the stroke patient makes voluntary elbow extension difficult or impossible. Activation of the triceps with electrical stimulation when a flexion synergy is present can be a means of generating latent elbow extension, inhibiting biceps spasticity & reducing the possibility of en elbow flexion contracture. Although symmetric biphasic waveform may be most comfortable […]
Read moreElectrical stimulation applied to the triceps muscle post stroke is useful to address a number of treatment goals including: preservation of elbow range of motion/prevention of biceps contracture, motor facilitation, reduction of upper limb flexor synergy & spasticity, weight bearing practice on the affected limb and overall improvement of upper limb alignment and posture. Patients […]
Read more
In post stroke gait – loss of ankle eversion can be a significant impediment to independent, safe gait as placement of the foot in a plantagrade position for weight bearing is lost. Loss of eversion may be seen in patients where tibialis anterior (ankle dorsiflexion) function is preserved and hip/knee function are within normal limits. […]
Read more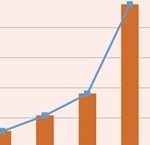
A 1999 study on stroke gait by Taylor et al., reported a mean 20 % gait speed increase in hemiplegic patients with use of the Odstock Dropped Foot Stimulator (ODFS). This finding has been supported in additional stroke gait studies comparing gait with and without FES intervention. Gait speed data obtained using APDM Mobility Lab […]
Read more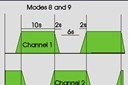
2 channel neuromuscular stimulation can be an effective intervention to reduce shoulder subluxation post stroke. Stimulation Delivery & Electrode Placement: Using the overlapping mode of the Odstock Microstim 2 channel exercise stimulator –one set of electrodes is placed over the anterior & posterior deltoid muscle and a second electrode set positioned over the middle deltoid & […]
Read more
A common assumption may be that fitting an ankle foot orthosis (AFO) is sufficient to address walking difficulty after neurologic impairment such as stroke, MS, traumatic brain or spinal cord injury. However, patients fitted with an AFO to assist walking can, in many cases, benefit from a foot drop stimulator as this intervention can be […]
Read more
In some individuals, MS may result in weakness of the lower limb (leg) muscles and difficulty with walking, Decreased walking endurance may also limit ability to walk even short distances out of doors or in the home. Through its effect in augmenting the force of a muscle contraction and eliciting movement lost due to MS, […]
Read more
Slow, inefficient gait with abnormal gait parameters are common findings when assessing walking post stroke. While loss of affected limb foot strike angle is a common finding we may additionally see compensatory change where foot strike angle in the non affected limb is similarly abnormal. Example 2 graph (grey area= normal range) illustrates the bilateral […]
Read more